
Integrating Computer
Facilitated Learning Resources into Problem-Based Learning Curricula
Gregor
E. Kennedy, The University of Melbourne
David M. Kennedy,
Monash University
Norm
Eizenberg, The University of Melbourne
Abstract
The focus of this
paper is on how computer facilitated learning (CFL) resources, if designed appropriately,
can be integrated with flexibility into problem-based learning (PBL) environments.
It takes as a case study the CFL program An@tomedia and the curriculum in the
School of Medicine at the University of Melbourne. The educational design of
An@tomedia, which emphasises integration between disciplines and a multiplicity
of perspectives, complements a number of teaching and learning modes within
the curriculum.
1. A Problem-Based Curriculum
In 1999, the School
of Medicine at the University of Melbourne introduced a new medical curriculum
incorporating problem-based learning (PBL), self-directed learning (SDL) and
educational technology (Keppell, Elliott & Harris, 1998). The introduction
of the new curriculum represented a fundamental shift in pedagogical focus for
the school. Traditionally, medicine had been taught using a discipline-based
approach with clear demarcation between the biomedical sciences on the one hand
(anatomy, biochemistry, physiology, etc.) and between biomedical and clinical
sciences on the other. Students would "cover" the basic sciences in
the first three years of their studies before "applying" their biomedical
science knowledge in the final three clinical years.
The introduction of PBL was seen as a way of addressing some of the problematic issues associated with traditional medical courses such as the artificial division between the biomedical (or basic) sciences and between the biomedical and clinical sciences. Koschmann, Kelson, Feltovich and Barrows (1996) argue that the division between basic science disciplines disguises the complexity and "ill-structured" nature of biomedical science knowledge. Furthermore, the division between biomedical and clinical sciences is of particular concern as students may spend a great amount of time learning material that is neither retained nor easily applied in their clinical years (Finucane, Johnson, & Prideaux, 1998; Koschmann, et al. 1996). Bowden and Marton (1998) note that "when medical graduates enter the workplace, they are not faced with situations labelled 'anatomy,' 'microbiology,' or the like. They are faced with patients with illnesses" (p. 129). In order to reconcile these difficulties, the new PBL curriculum was designed to provide horizontal integration across the various biomedical sciences and vertical integration of biomedical and clinical sciences.
The vehicle for integrating the various disciplines in the new medical curriculum is the "problem of the week." Each week students are presented with a clinical problem in a small group tutorial. Through group discussion and with the help of a tutor/facilitator, students generate hypotheses about the potential causes of the clinical problem. The group then considers the mechanisms that might underlie these hypotheses. This process allows students to identify aspects of the problem they think require further investigation over the week, which then become the students' "learning issues" for the week. The processes associated with exploring a problem require students to draw on biochemical, physiological and anatomical knowledge bases or a combination of these, which promotes the integration of biomedical science disciplines. Given that the problems of the week are usually clinically based, students are required to apply their biomedical knowledge in authentic clinical situations from an early stage in the curriculum.
Once students have completed their first PBL tutorial they are required to undertake SDL through which they investigate the weekly problem based on the learning issues they have generated. SDL is a student-centred approach to learning through which students take control of their own learning processes and experiences. The learners "decide how, where and when to learn the content they have identified as important" (Hammond & Collins, 1991, p. 153). A variety of resources are made available to students to support them in their SDL. Resources include more traditional modes of instruction (such as lectures and practicals) and electronic and paper-based resources (including text books, journal articles, web pages and computer facilitated learning (CFL) resources). Students use these resources to investigate their learning issues over the week, before returning to their second PBL tutorial where, as a group, they identify and discuss the critical mechanisms that underlie the problem. Through discussion, guided by the tutor/facilitator, students come to a resolution of the problem.
A critical feature of the new medical curriculum is the incorporation of educational technology to support student learning. The two major forms of educational technology employed are an online Course Management System (TopClass) and CFL resources (Keppell, Kennedy & Harris, 2000). TopClass allows students to access core content (problems of the week), send and receive mail, receive announcements from tutors and take online quizzes. CFL resources are used in areas where students traditionally have difficulties or in areas where the use of media, such as video, audio, high quality images or animation, is particularly appropriate to support students' understanding of concepts or principles. These resources may take a variety of forms including interactive multimedia programs, image banks, web sites and online resources such as biomedical atlases, encyclopaedias and dictionaries. The focus of this paper is on how one carefully designed multimedia program, called An@tomedia, has been successfully integrated into the new medical curriculum.
2. The Educational Design
of An@tomedia
An@tomedia is a multimedia program whose on-going development began five
years ago. It will be composed of eight modules, three of which (back, abdomen,
and thorax) have been completed and are currently used in the medical curriculum.
The program presently contains over 2000 high quality images and diagrams, including
radiographs, detailed dissection images of human bodies, and graphics with coloured
overlays highlighting key anatomical details.
An@tomedia allows students to explore anatomical concepts, principles and procedures from a variety of perspectives. The use of multiple perspectives (and multiple pathways) in CFL has been advocated because it allows learners to access the material in a manner more suited to their needs (Reeves, 1992). Individual differences in approaches to learning, prior knowledge and levels of interest lead students to approach an anatomical problem in a variety of ways. Moreover, Koschmann et al. (1996) argue that if students are provided with a single perspective, they may oversimplify concepts, which may ultimately prove misleading. Researchers have also advocated the use of multiple perspectives in teaching and learning as a support for higher levels of cognition, including reflective thinking (Ramsden, 1992; Laurillard, 1993).
Traditional models for teaching anatomy adopt either a systemic (e.g., nervous, musculo-skeletal, urinary) or a regional approach (e.g., back, pelvis, abdomen). The designers of An@tomedia integrated these two approaches, recognising that body systems pervade different regions of the body and that body regions are part of wider body systems. In addition to integrating these two perspectives, the developers identified the need to incorporate a strong practical dimension to the program. Practical work is a critical aspect of anatomy teaching and learning and has traditionally been taught using small group dissection classes. A less often used practical component of anatomy teaching and learning is imaging (CT scans, X-rays and MRI scans). In response to this practical component of anatomy, the developers included two further perspectives in the program: dissection and imaging. By incorporating these four perspectives in An@tomedia and by allowing students to move easily between them, the program attempts to link anatomical theory (regions and systems) with anatomical practice (imaging and dissection).
In addition to these four perspectives of anatomy, the developers recognised the need for a specific clinical focus in the program. In order to provide a comprehensive course in Anatomy, students must apply purely theoretical knowledge and practical discipline in clinical situations. Two strategies were used to promote clinical applications across all four anatomical perspectives. First, clinically-based questions were embedded within the program, focussing on the application of key anatomical concepts and principles in clinical situations. Second, a range of specific clinical techniques and procedures (such as where to perform a lumbar puncture) were embedded at appropriate points in the program.
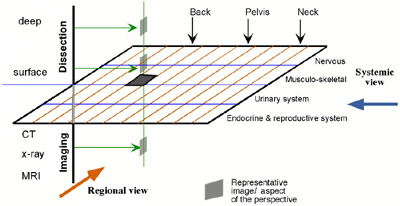
A summary of the educational approach adopted in the design of An@tomedia is presented in Figure 1, which shows a three-dimensional model of the program's educational design. The X-axis represents the anatomical regions (only three regions of the body are shown); the Y-axis represents anatomical systems (only four are shown); and the vertical axis represents the practical dimensions of dissection and imaging. Students may access anatomical content from any of these perspectives depending on their needs and interests. More importantly, once they begin investigating a particular content area, students can easily move between these perspectives. This is made clear in Figure 2 where the user is examining peripheral nerve supply from the "systems" perspective. The remaining three perspectives are listed on the lower right-reached with a simple mouse click.
Figure 1. The educational design of the An@tomedia showing the four perspectives
Figure 2 also gives an indication of the kinds of tasks and activities students can perform while exploring An@tomedia. They are challenged by both biomedical and clinical questions (e.g., "Can you identify the cutaneous territories supplied by thoracic, lumbar and sacral posterior rami?" or "Why may there be no detectable sensory loss following a lesion to a single posterior ramus?"). There are a variety of overlays of anatomical structures (muscles, nerves, fascia) that students may highlight for specific detail. Rollover points are also available so that students can easily identify particular anatomical structures on images. Finally, students are able to move between any of the modules in An@tomedia by clicking on regions of the human symbol in the bottom right corner of the screen.

Figure 2. A screen from An@tomedia showing the systems perspective, identification questions, clinically oriented questions and roll-overs
![]() An external link to the authors'Anatomedia startup screen with the four
prespectives shown.
An external link to the authors'Anatomedia startup screen with the four
prespectives shown.
From the explanation of An@tomedia's design, it should be clear that the program, while detailed and complex, is very flexible. This is an important attribute of the program given the pedagogical focus of the curriculum in which it is used. PBL and SDL are student-centred modes of relatively open and flexible instruction. The educational design of An@tomedia complements this pedagogical approach. The integrated approach adopted in the design and development of An@tomedia is analogous to the pedagogical approach being adopted in the School of Medicine. That is, the emphasis in both is placed on integration between disciplines and the need to consider multiple perspectives in exploring content. There is also a strong emphasis on the clinical application of basic science knowledge. Given the consistency of the curriculum's pedagogical focus and the educational design of An@tomedia, it was relatively easy to integrate the program into the medical curriculum. The following section details how An@tomedia has been used in the new medical curriculum at the University of Melbourne.
3. Using An@tomedia in a Problem-Based
Curriculum
An@tomedia has been used
as a resource in the problem-based medical curriculum in four ways:
As mentioned above, students are given access to a variety of CFL resources to assist them with their PBL and SDL. Students can access computer-based resources either in PBL tutorial rooms or in a biomedical computer lab, and An@tomedia is available for students in both these locations. In their PBL tutorials, students are able to use An@tomedia when discussing or reviewing anatomical principles or procedures relating to the problem. In addition, when undertaking their own SDL during the week, students can access An@tomedia to assist with their investigation of the problem. In this way An@tomedia is used as an invaluable resource to support students' PBL and SDL.
As part of their medical studies students complete theoretical anatomy tutorials and practicals on anatomy dissection and procedures. These two classes involve small group work with a tutor. In their theoretical classes, students are expected to form an understanding of anatomical systems and regions. More specifically, students are expected to be able to perform anatomical identification and clinical diagnosis as a result of completing this course. In their dissection and practical classes the focus is on dissection generally and anatomical procedures particularly related to the problems of the week. In both these classes An@tomedia is used as a preparatory tool for students. That is, students are asked to prepare for their theoretical and practical classes by covering relevant aspects of An@tomedia. Clearly the systems and regions perspectives are emphasised in the theoretical tutorials while the imaging and dissection perspectives are emphasised in the practical classes. In addition to being a preparatory tool, students are often asked to use An@tomedia as a review tool once classes have been completed. This allows students to review and reinforce key principles or procedures.
![]() n external link to the authors' demo on finding, comparing and contrasting anatomical
knowledge.
n external link to the authors' demo on finding, comparing and contrasting anatomical
knowledge.
The third use of An@tomedia involves traditional lectures. The examination and explanation of anatomical structures in lectures can be greatly enhanced through the use of An@tomedia. Lecturers are able to use the high quality diagrams, scans, and dissection images in An@tomedia as a tool for the explanation of concepts. Lecturers can easily and dynamically move between the systemic and regional views as well as through layered dissections to further enhance students' understanding of concepts and principles. By using An@tomedia as a lecturing tool, lecturers are able to familiarise students with the structure and navigation of the program, while simultaneously investigating anatomical content, which is relevant to the students' course and study goals.
Formative assessment, the fourth use of the program, is a key feature of An@tomedia. Students are frequently challenged with questions about the content they are reviewing. For example, students may be required to interpret a visual of a back dissection that displays the typical site of a bulging intervertebral disc compressing a particular lumbar spinal nerve. A range of relevant questions could be posed that will help students interpret the clinical symptoms and signs and relate them to the lesion displayed. Students can attempt to answer the questions in their notebooks and then access feedback in the form of an expert response to the question. They are also able to interact with images by using rollovers, which provide further explanatory and summary information.
![]() An external link to the authors' demo on a student view when using the module.
An external link to the authors' demo on a student view when using the module.
4. Evaluation of An@tomedia
An@tomedia has undergone extensive evaluation, both during its design and
development and after its implementation in the medical curriculum. Results
of these evaluations are reported elsewhere and will not be covered in detail
here (see Kennedy, Eizenberg & Kennedy, 2000a; Kennedy, Eizenberg &
Kennedy, 2000b). In these evaluations, data were collected from students and
anatomy tutors/lecturers using both qualitative and quantitative questions.
Quantitative responses were scored on five point likert scales (where 1 indicated
"strongly disagree" and 5 indicated "strongly agree"). Table
1 shows mean scores and standard deviations for items related to the interdisciplinary
design of An@tomedia. (Note that some questions were only asked of students
and others only of tutors). It can be seen from Table 1 that both students and
tutors were very positive about An@tomedia with mean scores for items typically
scoring above four.
![]() An external link to the AJET paper.
An external link to the AJET paper.
| Item | Mean (SD) | |
| Students (n=132) | Tutors (n=20) | |
| An@tomedia complements the anatomy teaching program. | 4.5 (0.71) | 4.60 (0.60) |
| The clinical applications seemed relevant and appropriate. | 3.9 (0.83) | 3.95 (1.18) |
| I found the ability to highlight structures in the images valuable. | 4.5 (0.67) | 4.75 (0.55) |
| I found the layering of images valuable. | 4.6 (0.69) | 4.84 (0.37) |
| An@tomedia helped me organise my knowledge of anatomy. | 3.8 (0.94) | |
| An@tomedia helped me understand anatomy from multiple perspectives. | 4.0 (0.78) | |
| An@tomedia enhanced my ability to interpret anatomy rather than merely describe it. | 4.0 (0.94) | |
| The four perspectives were well balanced and integrated. | 4.21 (0.71) | |
| After using An@tomedia students are likely to improve their knowledge of the anatomical basis of clinical procedures. | 4.15 (1.04) | |
| After using An@tomedia students are likely to improve their application of anatomical knowledge to solve clinical problems. | 4.00 (1.08) | |
Table 1. Mean scores and standard deviations for items relating to the educational design and integration of An@tomedia.
Tutors were also asked how they would like to see An@tomedia used for teaching and learning and were given space to write their responses. Ten tutors answered this question, and a summary of their responses is given in Table 2. An@tomedia was seen by a number of tutors as a useful tool in practicals and tutorials and as a resource for students in revision and in their SDL. Few tutors indicated they would direct students to the An@tomedia before their class and no tutors indicated they would use the resource as an explanatory tool in lectures. It should be noted, however, that many of the respondents in this group would not, in fact, give lectures in anatomy as this task would be carried out by only one or two lecturers.
| Tutors' suggested use of An@tomedia | Frequency |
| During practicals/tutorials | 4 |
| For a general revision/SDL | 4 |
| As a textbook style resource | 2 |
| As a complement to existing resources | 2 |
| Before practicals/tutorials | 1 |
| After practicals/tutorials | 1 |
Table 2. Tutors' suggested use of An@tomedia.
Students were also asked how they would prefer to use An@tomedia and were given four response options. Table 3 shows that while less than a third of students said they would find An@tomedia useful in lectures or tutorials, over half the students would use the program as part of group activities, and over 90% wanted their own copy of the program for SDL and revision. Given that student responses emphasize the use of An@tomedia as a SDL resource (either individually or in small groups), more background information may need to be given to users about the structure of the program and its potential uses.
| How would you best like to see An@tomedia used? | Frequency | % |
| Own copy for SDL and revision | 122 | 92.4 |
| Study groups | 70 | 53.0 |
| Tutorials | 43 | 32.6 |
| Lectures | 36 | 27.3 |
(1) Note that students could mark more than one response, meaning the sum of percentage scores is greater than 100.
Table 3. Students' preferences for the use of An@tomedia.
5. Conclusion
An@tomedia can be used to complement and support a variety of forms of teaching
and learning within PBL curricula. The flexibility inherent in the program has
ensured its effectiveness in various modes of instruction (PBL tutorials, SDL,
practical classes and lectures) at the University of Melbourne's School of Medicine.
This flexibility also allows An@tomedia to address different components of anatomy
(theoretical, practical and clinical). An@tomedia was not designed to replace
current forms of teaching and learning in anatomy, nor was it designed to become
the sole resource for the teaching of anatomy. Rather it was designed to complement
and extend current teaching of anatomy by providing new teaching and learning
opportunities for teachers and students alike.
6. References
Bowden, J., & Marton, F. (1998). The University of Learning: Beyond
quality and competence. London: Kogan Page Limited.
Finucane, P. M., Johnson, S. M., & Prideaux, D. J. (1998). Problem-based
learning: Its rationale and efficiency. Medical Journal of Australia, 168,
445-448.
Hammond, M. & Collins, R. (1991). Self-directed learning: Critical practice.
East Brunswick, N.J.: Nichols /GP Publishing.
Keppell, M. Elliott, K. & Harris, P. (1998). Problem based learning and
multimedia: Innovation for improved learning of medical concepts. In R.M.
Corderoy (Ed.) Proceedings of the fifteenth annual conference of Australian
Society for Computers in Tertiary Education (ASCILITE) (pp. 417-424). University
of Wollongong, NSW.
Keppell, M., Kennedy, G. & Harris, P. (2000). Transforming traditional
curricula: Enhancing medical education through multimedia and web-based resources.
In J. Bourdeau & R. Heller (Eds.) Proceedings of Ed-Media 2000 World Conference
on Educational Multimedia, Hypermedia and Telecommunications (pp. 1369-1370).
AACE. Charlottesville, USA.
Kennedy, D., Eizenberg, N., & Kennedy, G. (2000a). An evaluation of the
use of multiple perspectives in the design of computer facilitated learning.
Australian Journal of Educational Technology, 16 (1), 13-25
Kennedy, D, Eizenberg, N., & Kennedy, G. (2000b). An evaluation of interactive
multimedia designed to support problem based learning in medicine. In J.
Bourdeau & R. Heller (Eds.) Proceedings of Ed-Media 2000 World Conference
on Educational Multimedia, Hypermedia and Telecommunications (pp. 473-478).
AACE. Charlottesville. USA.
Koschmann, T., Kelson, A. C., Feltovich, P. J., & Barrows, H. S. (1996).
Computer-supported problem-based learning: A principled approach to the use
of computers in collaborative learning (pp.83-124). In T. Koschmann (Ed.), CSCL:
Theory & Practice in an Emerging Paradigm. Mahwah, Lawrence Erlbaum,
NJ.
Laurillard, D. (1993). Rethinking university teaching: A framework for the
effective use of educational technology. London: Routledge.
Ramsden, P. (1992). Learning to teach in higher education. London: Routledge.
Reeves, T. (1992, September-October). Effective dimensions of interactive
learning systems. In A. Holzl & D. Robb (Eds.), Finding the future:
ITTE '92, Proceedings of the Information Technology for Training and Education
Conference. Lucia, Brisbane: University of Queensland.
********** End of Document **********
| IMEJ multimedia team member assigned to this paper | Ching-Wan Yip |