| 1. | A Problem-Based Curriculum |
| 2. | The Educational Design of An@tomedia |
| 3. | Using An@tomedia in a Problem-Based Curriculum |
| 4. | Evaluation of An@tomedia |
| 5. | Conclusion |
| 6. | References |
![]()
Integrating Computer Facilitated Learning Resources into Problem-Based
Learning Curricula
Gregor
E. Kennedy, The University of Melbourne
David M. Kennedy,
Monash University
Norm
Eizenberg, The University of Melbourne
Abstract
The focus
of this paper is on how computer facilitated learning (CFL) resources,
if designed appropriately, can be integrated with flexibility into problem-based
learning (PBL) environments. It takes as a case study the CFL program
An@tomedia and the curriculum in the School of Medicine at the University
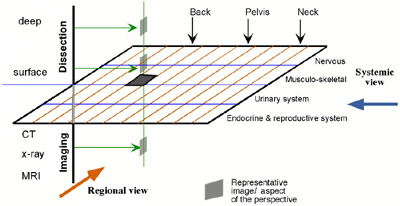
of Melbourne. The educational design of An@tomedia, which emphasises integration
between disciplines and a multiplicity of perspectives, complements a
number of teaching and learning modes within the curriculum.
1. A Problem-Based
Curriculum
In 1999,
the School of Medicine at the University of Melbourne introduced a new
medical curriculum incorporating problem-based learning (PBL), self-directed
learning (SDL) and educational technology (Keppell, Elliott & Harris,
1998). The introduction of the new curriculum represented a fundamental
shift in pedagogical focus for the school. Traditionally, medicine had
been taught using a discipline-based approach with clear demarcation between
the biomedical sciences on the one hand (anatomy, biochemistry, physiology,
etc.) and between biomedical and clinical sciences on the other. Students
would "cover" the basic sciences in the first three years of
their studies before "applying" their biomedical science knowledge
in the final three clinical years.
The introduction of PBL was seen as a way of addressing some of the problematic issues associated with traditional medical courses such as the artificial division between the biomedical (or basic) sciences and between the biomedical and clinical sciences. Koschmann, Kelson, Feltovich and Barrows (1996) argue that the division between basic science disciplines disguises the complexity and "ill-structured" nature of biomedical science knowledge. Furthermore, the division between biomedical and clinical sciences is of particular concern as students may spend a great amount of time learning material that is neither retained nor easily applied in their clinical years (Finucane, Johnson, & Prideaux, 1998; Koschmann, et al. 1996). Bowden and Marton (1998) note that "when medical graduates enter the workplace, they are not faced with situations labelled 'anatomy,' 'microbiology,' or the like. They are faced with patients with illnesses" (p. 129). In order to reconcile these difficulties, the new PBL curriculum was designed to provide horizontal integration across the various biomedical sciences and vertical integration of biomedical and clinical sciences.
The vehicle for integrating the various disciplines in the new medical curriculum is the "problem of the week." Each week students are presented with a clinical problem in a small group tutorial. Through group discussion and with the help of a tutor/facilitator, students generate hypotheses about the potential causes of the clinical problem. The group then considers the mechanisms that might underlie these hypotheses. This process allows students to identify aspects of the problem they think require further investigation over the week, which then become the students' "learning issues" for the week. The processes associated with exploring a problem require students to draw on biochemical, physiological and anatomical knowledge bases or a combination of these, which promotes the integration of biomedical science disciplines. Given that the problems of the week are usually clinically based, students are required to apply their biomedical knowledge in authentic clinical situations from an early stage in the curriculum.
Once students have completed their first PBL tutorial they are required to undertake SDL through which they investigate the weekly problem based on the learning issues they have generated. SDL is a student-centred approach to learning through which students take control of their own learning processes and experiences. The learners "decide how, where and when to learn the content they have identified as important" (Hammond & Collins, 1991, p. 153). A variety of resources are made available to students to support them in their SDL. Resources include more traditional modes of instruction (such as lectures and practicals) and electronic and paper-based resources (including text books, journal articles, web pages and computer facilitated learning (CFL) resources). Students use these resources to investigate their learning issues over the week, before returning to their second PBL tutorial where, as a group, they identify and discuss the critical mechanisms that underlie the problem. Through discussion, guided by the tutor/facilitator, students come to a resolution of the problem.
A critical feature of the new medical curriculum is the incorporation of educational technology to support student learning. The two major forms of educational technology employed are an online Course Management System (TopClass) and CFL resources (Keppell, Kennedy & Harris, 2000). TopClass allows students to access core content (problems of the week), send and receive mail, receive announcements from tutors and take online quizzes. CFL resources are used in areas where students traditionally have difficulties or in areas where the use of media, such as video, audio, high quality images or animation, is particularly appropriate to support students' understanding of concepts or principles. These resources may take a variety of forms including interactive multimedia programs, image banks, web sites and online resources such as biomedical atlases, encyclopaedias and dictionaries. The focus of this paper is on how one carefully designed multimedia program, called An@tomedia, has been successfully integrated into the new medical curriculum.
![]()